

The Big Idea
Q. How can physicians help Parkinson’s patients when medications fail?
A. A new surgery, Deep Brain Stimulation, has had dramatic results.
For years, life with Parkinson’s disease had been challenging but manageable for Steve Blevins because of the medications that kept his symptoms under control. But there came a time when the drugs weren’t working consistently and he found himself once again struggling with buttons, zippers and other everyday movements that normally would be routine.
That’s when he turned to Deep Brain Stimulation, a brain surgery for Parkinson’s that has made major advancements in recent years. Blevins is an internal medicine physician at OU Health, where neurosurgeons and neurologists are expanding a program that is vastly improving the quality of life for people with Parkinson’s. Since Blevins underwent the surgery—which involves placing electrodes deep into the brain—he has regained the joy of movement once thought lost for good.
“I’m very passionate about Deep Brain Stimulation (DBS) for people with Parkinson’s because it dramatically helps with their motor symptoms,” says OU Health neurosurgeon Andrew Conner, M.D., who performed the surgery on Blevins. “DBS does not slow the progression of the disease, but it returns function and quality of life for the vast majority of patients.”
Blevins was diagnosed with Parkinson’s disease 13 years ago. For years, the standard drug combination of levodopa-carbidopa worked wonderfully, allowing him to continue his work as a doctor and medical educator. But eventually he began having “motor fluctuations,” in which his medications worked unpredictably and his symptoms returned. Increasing his dosage only caused more side effects, which can include nausea, vomiting and low blood pressure. He reached a point where he felt medication itself was no longer beneficial.
“I had regressed to an earlier time when I couldn’t hold my right arm normally or use my fingers and hands properly,” Blevins says. “I was walking on the sides of my feet instead of the soles of my feet. As my quality of life declined, I said, ‘It’s time to operate on me.’ ”
Treating patients with DBS requires physicians in two specialties: neurosurgery and neurology. As a neurosurgeon, Conner’s expertise is implanting the electrodes, a procedure that requires great precision to reach desired targets in the brain. After the surgery, the patient moves to the care of a neurologist, who programs the implanted device to achieve symptom control.
Once a patient is verified as a candidate for DBS, Conner determines whether the surgery will take place while the patient is awake or under general anesthesia, the latter being far more common than in years past when a patient needed to be awake so that the surgeon could find the correct targets for the electrodes.
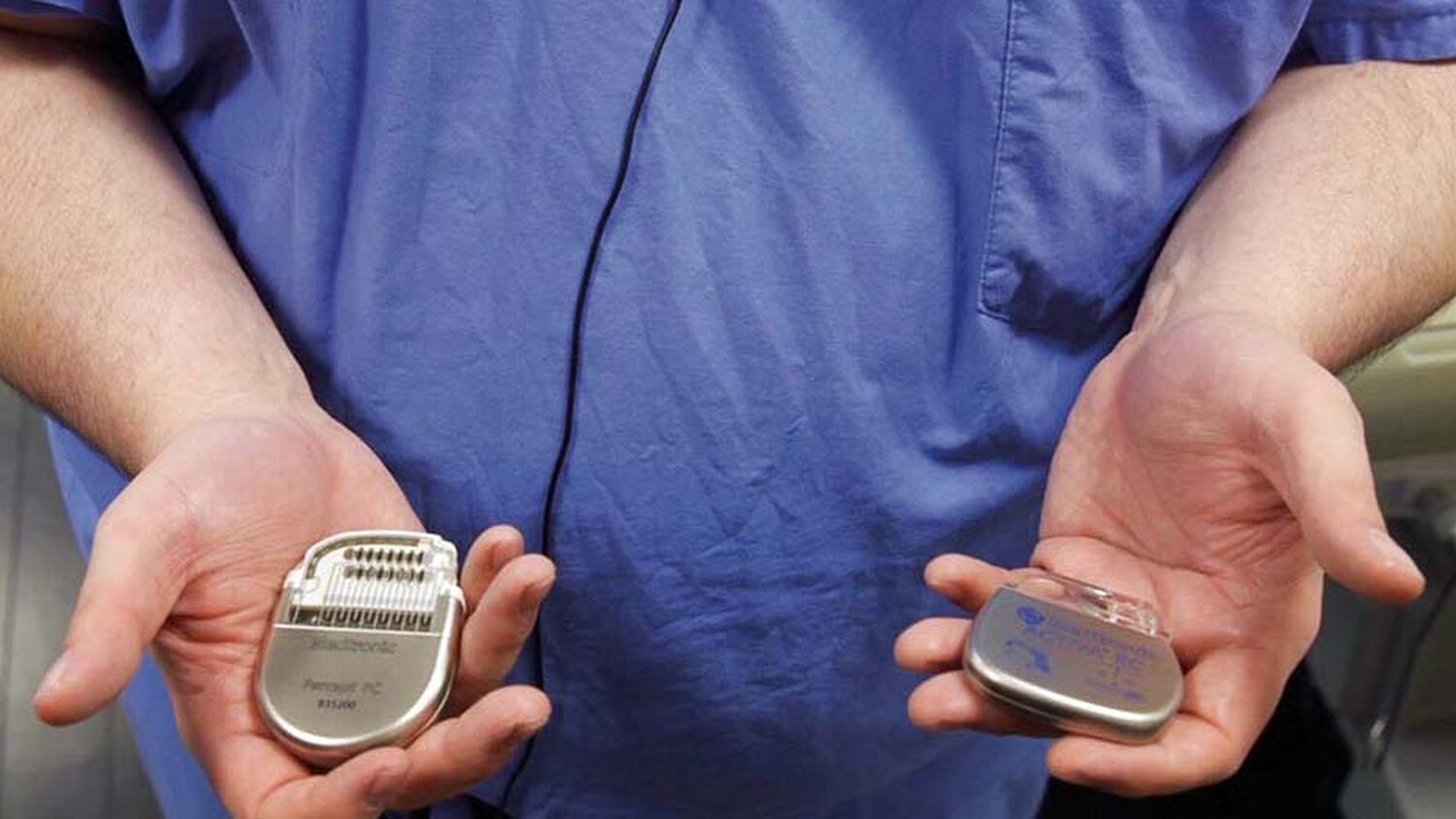
Today, the target locations in the brain are confirmed using magnetic resonance imaging (MRI) while the patient is under anesthesia. After securing the patient’s head, the surgical team moves the patient in and out of the MRI scanner to find and confirm the two targets, called STN (subthalamic nucleus) and GPi (globus pallidus internus), which are responsible for movement control. Behind the hairline, holes are drilled, the openings a bit smaller than a quarter, and the electrodes are inserted to the target locations. Patients generally stay in the ICU a day or two before going home, but a week later they return for a shorter outpatient procedure to implant a battery pack. The battery is connected to the electrodes through extension wires and the pack is placed under the skin below the collarbone.

“DBS is a joint process with the rologist. I implant the electrodes and the neurologist programs the device,” says Conner, who did his fellowship training at the University of California San Francisco, which pioneered the use of MRI-guided DBS. “Most patients receive extremely good benefits. It’s very gratifying to see them gain their function back.”
While medications for Parkinson’s help the brain to replenish its supply of dopamine, DBS works by using electrical signaling to stimulate the neurons that contain dopamine, thereby controlling a patient’s symptoms. Programming a patient’s DBS device is a meticulous and ongoing process, says OU Health neurologist Faiza Butt, M.D., who did her fellowship training with Conner and joined the team last year on the Oklahoma City campus.
She typically begins programming the patient’s device in her clinic within a month of surgery, adjusting the voltage, pulse width and frequency to address a patient’s specific symptoms. DBS is often effective for patients with medication-resistant tremors; dyskinesia, or involuntary movements; and dystonia, in which muscles contract involuntarily, causing repetitive or twisting movements.
“DBS is a great treatment for patients when their medications are no longer controlling their symptoms sufficiently or they are having severe side effects from the medication,” Butt says.
Many patients who undergo DBS for Parkinson’s are able to significantly lower their medication dosage, says Syed Hussain, M.D., an OU Health neurologist in Tulsa. DBS is also a long-term treatment, only requiring new batteries from time to time. Because there are four points of stimulation on each electrode implanted on either side of the brain, there are numerous combinations to use, if needed, Hussain says.
“I have never had a patient reach a point where DBS is no longer beneficial,” Hussain says. “It works 24/7 and controls most symptoms, and many patients can reduce their medications once they reach a good setting. Their walking improves and comes naturally. They’re often able to resume hobbies with their families and friends. It can be like turning the clock back 10 years.”
Blevins is grateful to have his quality of life back and to have renewed vigor for his work, which involves teaching residents and enhancing the curriculum as associate dean for medical education in the OU College of Medicine.
“I’ve had a lot of improvements, for which I am very grateful,” Blevins says. “DBS is not curative for Parkinson’s, nor does it necessarily slow down its progression, but the benefits are tremendous.”
April Wilkerson is a writer and editor for OU Health.
To comment on this story, click here.