


Not in Vain
After the death of a patient, a young doctor promised to find a more efficient way to identify remaining cancer cells in the body.
You might say that Dr. Jennifer Holter Chakrabarty has been walking around with a chip on her shoulder for well over a decade.
The associate professor of medicine and bone marrow transplant physician at the Stephenson Cancer Center on the University of Oklahoma Health Sciences Center campus is the type of doctor who takes losses personally, and in the high-stakes world of hematology and oncology, that can mean a lost life, a motherless child and a family tragedy. Those are memories she carries with her and that drive her. She still talks about a particular case she had in 2006, when her medical career was still young.
The leukemia patient ultimately died of a fungal infection she contracted following a bone-marrow transplant. Leukemia is a type of cancer that attacks the marrow within a person’s bone structure. Doctors typically fight it with chemotherapy treatments that kill the cancer along with the patient’s marrow.
Bone marrow plays a critical role in the body, serving as the major factory for everything in the blood, such as red blood cells that carry oxygen and white blood cells that fight infection.

Holter Chakrabarty was the physician who conducted the woman’s infusion of new bone marrow cells, and she worked with her patient through an agonizing, four-week period, waiting for the marrow to be fully functional. In the meantime, she administered an assortment of infection-fighting medications and treatments needed to compensate for the patient’s depleted immune system.
Transplant patients walk a delicate tightrope, and failures sometimes happen even though the medical team does everything possible to prevent them. All components within the infused marrow must function in balance, and Holter Chakrabarty says there are two fundamental components in play. There is stroma, which Holter Chakrabarty describes as the soil, and there are stem cells, which she calls the seeds. Those stem cells derive their nourishment from stroma, much like seeds derive nourishment from soil.
If they work together properly, those seeds produce the blood cells the body depends on. If one or the other fails, the marrow is not productive, and it can be increasingly vulnerable to bacteria, viruses and disease and require repeated transfusions of blood and platelets. As with actual soil and seeds, another component of growth is time, and in the case of bone marrow, doctors must wait 28 days before they can be certain of a transplantation’s success.
Over that period, a patient can be vulnerable to a multitude of invaders with no natural defense system. That’s what claimed Holter Chakrabarty’s patient in 2006. If only there would have been more warning time. If she could have had a clearer picture of the new marrow’s development, measures could have been taken, and her life might have been saved.
The loss was devastating for Holter Chakrabarty, the type of emotional blow Dr. Robert Epstein had seen before in his colleagues.
“It was normal,” he says. “We all wish we could have done something different when things didn’t work out.”
As an OU medical school professor and a specialist in hematology and oncology, Epstein stayed current on medical research literature, and had been reading about work with a new radioactive imaging biomarker developed to help spot cancer through CT and PET imaging scans. He passed the paper to Holter Chakrabarty and suggested that it might just contain a solution to her problem. As he had with other young doctors, Epstein encouraged Holter Chakrabarty to follow up and work on a solution other doctors could use in similar situations.
Holter Chakrabarty, who holds the Inasmuch Foundation Chair in Cancer Screening, Education and Outreach, was determined to do something to ensure her patient’s death would not be in vain, so she began looking into the new imaging isotope, known as Fluorothymidine, or 18 F-FLT. When it was first developed, the biomarker was an exciting new imaging agent that could be injected into the body to help doctors spot cancerous tissue more easily through diagnostic testing.
The problem was that it did its job too well, Holter Chakrabarty says. Scans using the biomarker showed bone marrow within the patient’s skeletal frame, blocking the view of other organs.
“If I were a breast cancer surgeon, I couldn’t see because the bones in the chest got in the way of the breast tissue, and it occluded my ability to see the breast cancer,” she says.
But for Holter Chakrabarty, the technology had breakthrough potential because, for the first time, she could actually see the bone marrow with which she worked.
Although the isotope had been developed by 2001, it had not yet been widely studied in 2006 because bone marrow disorders are relatively rare compared to breast cancer, lung cancer and other diseases.
But for Holter Chakrabarty, and a small cadre of colleagues in her field, FLT represented a transformational development that could save lives. Under current clinical practice, bone marrow is largely monitored through biopsies, which require needles to extract marrow samples from specific bone locations, and marrow extracted from only a few points doesn’t always reveal a complete picture of marrow within the entire organ.
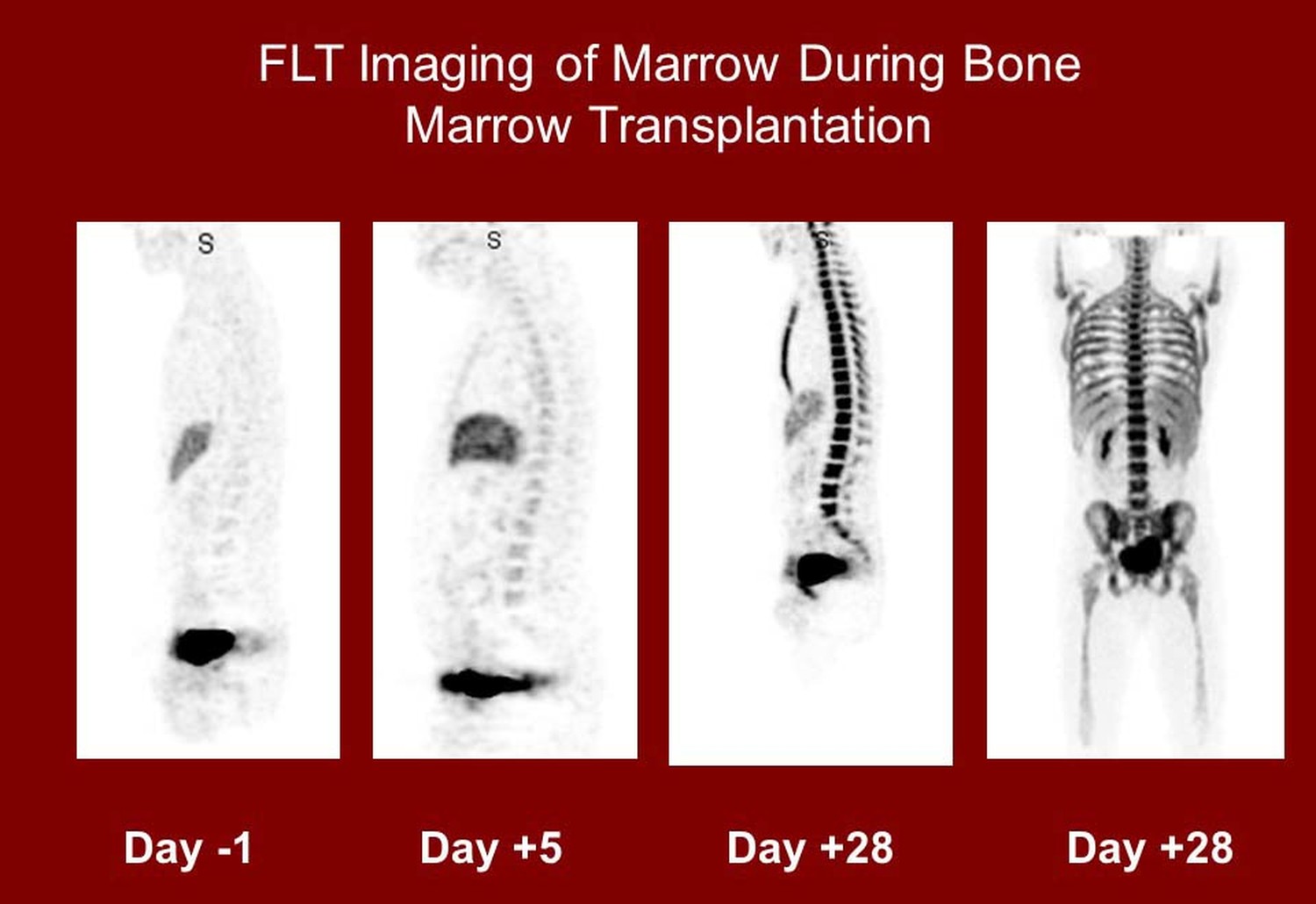
Using FLT, doctors could have a much larger window into the entire marrow cavity, and they could have a clear view of bone marrow within the spine, sternum and other bones in the body that are not easily accessible. That clear view could allow Holter Chakrabarty and other doctors a non-invasive way to monitor bone marrow infusions within days after they are administered.
That’s important because FLT could provide a quicker way to determine whether a patient’s marrow is alive and growing, or if it’s non-functional, giving doctors a head start on measures that could save a patient’s life, Holter Chakrabarty says.
“The breakthrough technology of FLT could be “the difference between five days and 28 days” in knowing if cancer has been eradicated and bone marrow is returning, says Dr. Jennifer Holter Chakrabarty.”
While the development of FLT technology was exciting news for Holter Chakrabarty and her colleagues in 2006, it only marked the beginning of a long research effort to prove that it really could be transformational for patients with leukemia and other bone marrow diseases.
They had only recognized the potential, but there had been no research to determine if it was safe or effective, so they began a journey of research and collaboration with lab animals, and that now continues with a clinical study involving humans.
Using rats, Holter Chakrabarty says she demonstrated that the FLT biomarker could be used to differentiate between bone marrow that was alive and growing and marrow that was killed by radiation exposure, such as in a radiation event.
First, she radiated her test animals, then infused new marrow cells into their bodies and watched the progression, using scans with the new FLT biomarker.
“I did that, and I could tell the difference between the two groups within four days,” she says. “I could tell who was going to live and who was going to die, because if your marrow repopulates, you’re going to live.”
As research associated with FLT’s clinical viability has continued, Holter Chakrabarty has been collaborating with OU electrical engineers and bioengineers on a parallel project they hope will open the door to faster, more accurate analysis of CT and PET scans involving the biomarker.
OU engineers Joseph Havlicek and Chuong Nguyen are using computer and machine learning technology to develop algorithms that can search CT and PET scans for cancerous cells within the body’s marrow cavity.
It’s a project the three have been working on since they met at an event for undergraduates five years ago. The engineers say their technology can analyze an entire scan and deliver thorough, accurate results within five minutes, a task that can now take hours with conventional technology.
“There’s a lot of machine learning or artificial intelligence work being done to enhance the analysis of mammography and other kinds of scans, but we’re the only people we know of who are working on this for leukemia patients.” Havlicek says. “We’re the only ones working on bone marrow transplant patients specifically, and we’re the only ones working with this new FLT biomarker.”
Nguyen and Havlicek say they still see opportunities to make their algorithms faster and more accurate while Holter Chakrabarty and her medical colleagues continue their work with FLT. At some point, they plan to launch the technology into the commercial market.
“We hope this will replace the current kind of software that is laborious and time consuming with a widespread commercial product that goes into every scanner in the country,” Havlicek says.
In the next phase of FLT research, Holter Chakrabarty will analyze bone marrow scans taken from humans using the FLT isotope. That work is just getting under way and could take five years to complete.
If their results clear a path to clinical applications, she says FLT could be an enormous step forward in the fight against leukemia.
“If I could see leukemia, I could more accurately choose where I put a needle, so I could actually identify disease better, and that would be an added benefit. Better identification and quantification may lead to new ways of thinking about leukemia, and hopefully better therapies.
“But it all has to be proven,” she says. “There’s a huge amount of work left to do.”
But, to Epstein, the mentor who first introduced Holter Chakrabarty to FLT, her work is already invaluable because it could some day make it easier for doctors to estimate bone marrow growth, and that’s what he asked her to do when he handed her that research paper in 2006.
While work is far from over, Holter Chakrabarty acknowledges that much has already been accomplished. She has published research on FLT, grants have been obtained and all that momentum is carrying FLT research closer to the finish line.
“I told my kids and my husband and Dr. Epstein that before I finish my career, I was going to contact that family and tell them that her death was not in vain. And, that I had done something to make sure that was not the case.
“Now I can say I’ve kept that promise.”
Chip Minty is a Norman-based writer and the principal of Minty Communications, LLC.
To leave a comment on this story, click here.