

OU-Tulsa's Culinary Medicine Program
helping doctors treat the root of many life-threatning diseases through proper nutrition
The vegan eggplant lasagna was the favorite dish among the eight future physicians who cooked together during spring semester finals week. But this was no ordinary potluck. The students were finishing a culinary medicine course offered on the University of Oklahoma’s Tulsa campus.
Each prepared a recipe specifically to treat diabetes: homemade, high-fiber flatbread with Moroccan carrots and lentils; black bean patties with rainbow slaw; grilled cauliflower steak with chimichurri sauce; and baked apples with cinnamon-nut filling.

Before taking the course, Ian Peake, a first-year medical student, had never even chopped an onion. Now he can explain why lemon juice is a good replacement for salt while he spiral cuts a cucumber for an Asian-inspired salad.
“I wanted to learn more about nutrition and food,” Peake says. “As a future doctor, I can’t tell people to eat better and expect them to know how, especially if I didn’t know how. We need more programs like this and to be able to prescribe food like we would prescribe medication.”
For two years, a culinary medicine curriculum has been available to medical students in the OU-TU School of Community Medicine (SCM). The hands-on pilot program, funded by the Ardmore Institute of Health, the Oxley Foundation and the Hille Foundation, teaches students how to cook and prescribe foods designed for various chronic diseases. It is part of the “lifestyle medicine” specialty, which is undergoing a national growth explosion.

Though voluntary, the SCM culinary medicine program received 100 percent medical student participation. It became so wildly popular that the number of classes was doubled to meet demand.
So far, nearly 100 classes have been held for more than 250 healthcare students and professionals and an additional 250 community members. Participants include students in OU medicine, physician assistant and public health programs, along with OU-Tulsa employees and community members.
This success has led to further expansion this fall, when lifestyle medicine becomes part of SCM’s required curriculum. SCM will be among the first medical schools in the United States to fully integrate the specialty. The school was also the first in the nation to require that all physician assistant students complete the course for graduation.
OU’s new culinary medicine program was developed by a three-person, multi-disciplinary team — emergency room physician Dr. Lori Whelan, registered dietitian Marianna Wetherill, Ph.D., and Chef Valarie Carter.
Whelan is an emergency physician at Hillcrest Medical Center, OU-Tulsa associate professor in emergency medicine and a George Kaiser Family Foundation Chair in emergency medicine. She has been patching up the effects of poor health in emergency rooms for more than 20 years.
“The state of our health is horrible in Oklahoma,” Whelan says. “I always tell people that in the emergency room, the faucets are on and overflowing, and I’m constantly mopping. I want to do what I can to turn off the faucets.”
Oklahoma’s health statistics are among the most serious in the nation. About 37 percent of adult residents are obese (No. 3), 33 percent are physically inactive (No. 3), 13 percent have diabetes (No. 8) and 12 percent smoke (No. 12), according to America’s Health Rankings from the United Health Foundation. Oklahoma also has the third-highest rate of cardiovascular deaths, sixth-highest in cancer deaths and the seventh-highest infant mortality rate.
“I had no nutritional education in medical school or any type of lifestyle intervention training as a doctor or resident,” Whelan says. “There is a lot of literature showing the power of ‘lifestyle medicine’ as a basis for treating patients and trying to get at the root cause of the problem.”
For eight years, Whelan has personally adhered to a whole-food, plant-based diet and counseled emergency-room patients on lifestyle behaviors, but had not formally taught her students, nor researched culinary medicine.
“I felt embarrassed as a physician that I wasn’t aware of this and wanted to educate medical students, residents and other physicians on the power of food as medicine and how lifestyle changes can improve chronic disease,” says Whelan.
Lifestyle medicine offers treatment, reversal and prevention of chronic diseases through evidence-based dietary and behavior changes. Simple dietary changes can treat at-risk conditions, including cardiovascular and renal disease, diabetes, allergy and autoimmune deficiencies, pregnancy, early childhood, arthritis, mental health and gastrointestinal issues.
About 300 physicians have earned their certification in lifestyle medicine since the American Board of Lifestyle Medicine began offering it in October 2017.
The new SCM program trains students how to incorporate six evidence-based lifestyle behaviors into a patient’s evaluation and treatment plan: nutrition, exercise, stress management, sleep, healthy relationships and substance-use cessation.
“Every physician needs to understand the role these lifestyle behaviors have on the disease process,” Whelan says. “If food is medicine — and I believe it is — and doctors are the experts in medicine, then we need to be the experts in food.

“The more we understand what certain nutrients are in each food and how to put those foods together into a delicious meal, then we are giving ourselves medicine.”
Prior to the pilot program, the only nutrition information was provided to students in a few short lectures, which is typical in medical schools. With so much coursework to cover, medical schools slowly pushed nutrition and lifestyle to the background.
An OU-Tulsa dietician, Wetherill is also an assistant professor in the OU Hudson College of Public Health and the School of Community Medicine, and holds the George Kaiser Family Foundation chair in population healthcare. She brought up the need for a nutrition curriculum about six years ago.
Wetherill began her efforts with an annual nutrition presentation for third-year medical students and says they always had more questions and requests for resources. In 2017, medical students requested a healthy cooking class that soon filled to capacity. This enthusiasm confirmed the need and interest for a broader culinary medicine initiative.
“Medical students are very enthusiastic about preventive health and lifestyle medicine coming into medical school. In fact, many of them expect it,” Wetherill says. “But, as they go through training, these topics are often an afterthought, if at all, which sends a message to our future physicians that lifestyle has little role to play in the cause and treatment of chronic disease.”
Patient empowerment through nutrition and other lifestyle changes has been a passion for Wetherill, who helped push lifestyle-medicine requirements for the physician assistant program.
“This is where you start to change culture; when a medical school is bold enough to recognize lifestyle medicine as a discipline, and chooses to teach its students how it can be used as a fundamental part of a patient’s treatment plan,” Wetherill says.

Eighty to 85 percent of a person’s health is determined by factors outside healthcare. Lifestyle medicine gives healthcare providers the additional tools necessary to address these factors, she says.
“In medical school, we spend months and months teaching students about pharmacology,” says Whelan. “That is why we decided to integrate a curriculum that spends as much time on food and nutrients as we do on pharmacology.”
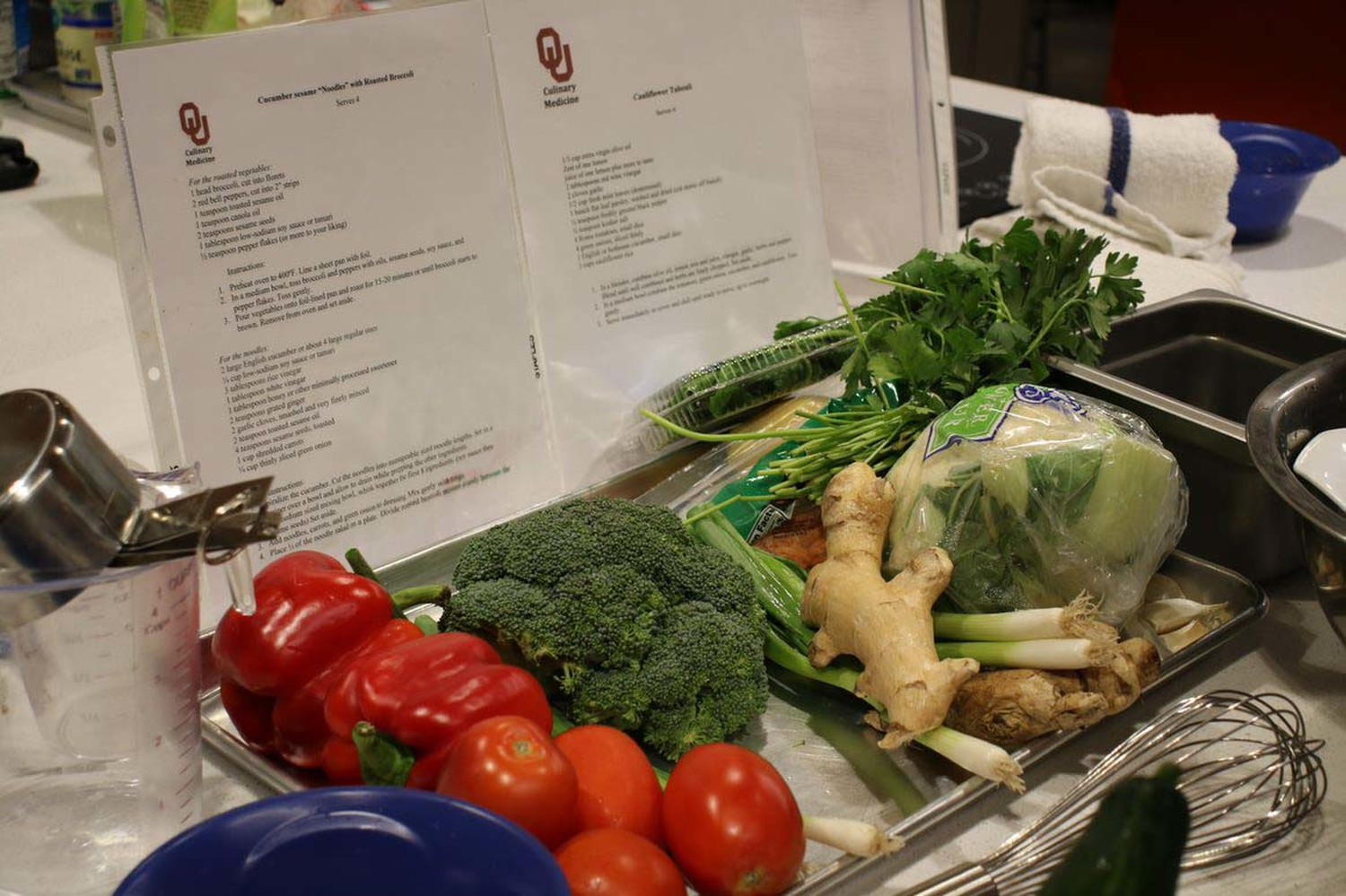
Chef Valarie Carter co-facilitates the culinary medicine classes and develops recipes as part of the teaching team. Wetherill provides her with an “ingredient wish list” proven effective in treating specific disorders, then Chef Carter creates 10 to 12 recipes for the cooking module based on goals for a particular health condition.
Carter holds a plant-based nutrition certification from Cornell University and is currently completing her Master’s in Public Health (MPH) at OU-Tulsa. Previously, she consulted with school districts and youth programs to revamp healthful menus for kid appeal.
“At this point in my life, I am very interested in being able to improve people’s lives through food,” Carter says. “I want people to get these really basic skills that can change their lives. They are small changes that can make huge differences.”
Students are finding their own behaviors evolving as they take classes.
John Carradini, a fourth-year medical student who completed his MPH at OU-Tulsa earlier this year, says he grew up on a typical meat-and-potatoes diet and didn’t cook much.
“Most of my classmates had similar backgrounds, and during medical school, cooking was an inconvenient thing you had to do in between studying,” Carradini says. “After our culinary medicine classes, we’re cooking more and now understand how foods work together.
“These classes make students more comfortable counseling about nutrition and more comfortable trying foods they haven’t tried before. They look at healthcare in a different way.”
As an MPH student, Carradini worked as a research assistant on the evaluation of the program. A paper he had published in Medical Science Educator showed that physician-assistant students who completed the classes gained more nutritional knowledge and counseling confidence than a control group.
“Nutrition is not commonly talked about among students,” Carradini says. “We have curriculum about alcohol and tobacco, but we don’t get a lot of nutritional information. We are largely undereducated about nutrition, which is problematic to our future practice, but thankfully, our education is growing.”
Affordability for patients is a big part of lifestyle medicine.
“If we want to improve the health of entire communities, then health equity must be part of the conversation,” Wetherill says. “We need to get to a place where providers can speak to all patients, regardless of their walks of life, and provide them with the support necessary to make behaviors change,” Wetherill says. “In the context of lower-income patients, training physicians on making referrals to healthy food assistance programs or sliding-scale exercise programs is an important part.”
Research assistant Victoria Thomas, a fourth-year medical student who recently completed her MPH, says she used to search for healthy diets online before culinary medicine was offered.
Thomas says earlier coursework on metabolism had mentioned Dietary Approaches for Stopping Hypertension (DASH) and Mediterranean diets, but no details or demonstrations were provided.
“This is a huge positive for OU-Tulsa,” Thomas says. “It sets us apart from any other program in the state and provides hands-on learning and practical experiences instead of theoretical bookwork.”

Whelan likens the emphasis toward lifestyle medicine to how other infectious disease epidemics are treated.
“Say we have an E-coli outbreak. We don’t spend billions of dollars creating new medications to deal with the symptoms,” Whelan says. “We spend time and money tracking down the source of the problem and eliminating it.
“A lot of these chronic illnesses should be considered food-borne illnesses. We are trying to treat them with pills rather than addressing the root cause. So many outcomes of these chronic diseases cannot only be significantly improved, but in many cases can also be completely reversed or cured by changing the food we are eating.”
Rather than simply advising a patient to lose weight, get more exercise or reduce stress, lifestyle medicine brings specificity, clarity and self-empowerment to a patient, Whelan says.
“We are training our students not only to give lifestyle prescriptions, but also to work with patients and support them while making these lifestyle behavior changes,” she adds.
Data has shown significant improvement — and sometimes reversal — of many chronic diseases when lifestyle changes are made. The movement also calls for incorporating lifestyle medicine questions into all segments of health care, just as it does with tobacco use.
“There is no patient I see without asking if they smoke,” says Whelan. “It has taken years, but we know it is such a public health problem that we finally got to the point where we ask every patient if they use tobacco. That is the model needed for nutrition and other lifestyle behaviors.”
This doesn’t mean physicians would handle everything. Lifestyle medicine requires interdisciplinary collaboration through group medical visits, in-office dietitian services, and integrated referral systems that connect patients with community resources needed for ongoing behavior change.
“I tell students I don’t expect them to personally do all of the lifestyle counseling a patient may require, but they are the captains setting the course for the overall treatment plan. They need to center lifestyle as a priority in their practice and leverage the skillsets of an interdisciplinary team to help patients reach a destination toward healing,” Whelan says.
“As an ER doctor, I have less time than anyone to talk to a patient about what they are eating, how much they are sleeping, or if they are getting physical exercise. But if I can make time, anybody can.”
A long-term goal of the team is to create a lifestyle medicine institute on campus to coordinate research and interventions in areas such as nutrition, sleep, stress management and physical activity.
“It would bring together our collective expertise to achieve a greater goal,” Whelan says. “For OU to be part of this movement is very exciting.”
Ginnie Graham is a reporter for the Tulsa World.
Photos by Amanda Murphy, OU-Tulsa.
To comment on this story, click here.